











What are those bumps on my child's skin?
It’s common for children to develop a condition that causes a rash. Here’s a guide to 12 conditions that dermatologists frequently see that can cause a rash of bumps on your child’s skin.

Acne
What you may see: Blackheads, whiteheads, and pimples may appear on your child’s skin at birth or shortly afterward.
Contagious: No.
Is treatment necessary? Acne that begins between birth and 6 weeks goes away on its own without treatment. When acne begins after 6 weeks of age and before puberty, it’s best to see a dermatologist.
Warning
Never apply acne medication to your child’s skin unless a dermatologist recommends it. A baby’s skin is very sensitive.
Related AAD resource:
Atopic dermatitis

Atopic dermatitis (AD), which is often called eczema, is common in children.
Contagious: No.
Is treatment necessary? The AAD recommends seeing a board-certified dermatologist to make sure your child has this condition. AD can come and go for years. Proper treatment can prevent the condition from worsening and ease the itch.
Related AAD resource:
Contact dermatitis

Diaper rash is a type of contact dermatitis. Many other everyday things, including musical instruments, can also cause this condition. With so many causes, it can take time and the expertise of a dermatologist to find the cause(s).
Contagious: No.
Is treatment necessary? To get relief, your child must avoid what causes the rash. You may also need to treat the rash for it to clear. A board-certified dermatologist can help you:
Find the cause of the rash (This can take time.)
Tell you what to avoid
Determine whether treatment is needed to clear the rash.
Related AAD resource:
Folliculitis

Is it contagious? No.
Is treatment needed? When you avoid what’s causing the bumps, folliculitis generally clears on its own. In babies and children, the cause is often tight clothing.
Related AAD resource:
Hand-foot-and-mouth disease

Contagious: Yes. A virus causes hand-foot-and-mouth disease (HFMD). Most people get HFMD by 5 years of age.
Is treatment necessary? HFMD tends to clear on its own without treatment in 7 to 10 days. If your child gets HFMD before 2 years of age, it can take longer for your child to feel better.
It’s important to keep your child at home while your child has bumps and blisters and symptoms, such as fever. This helps your child recover and prevent spreading the disease to other children. At-home treatment can help relieve symptoms, such as painful mouth sores and fever.
Related AAD resource:
Heat rash
Contagious: No.
Is treatment needed? If your child has a heat rash, take your child to a cool place. This will help stop the sweating, allowing the rash to go away on its own in a few days. Your child will also feel more comfortable. If you still see the rash after a few days, call your pediatrician or a board-certified dermatologist.
Hives

Contagious: No.
Is treatment necessary? Hives tend to appear and clear within a few hours. Your child may get hives once and never again. It’s also possible to have many flare-ups. If your child continues to get hives daily or almost every day for six weeks or longer, your child has a condition called chronic hives. Getting relief often requires medical help. A board-certified dermatologist can tell you whether your child has hives or another condition.
Related AAD resources:
Impetigo

Contagious: Yes. All types of impetigo are very contagious. It is caused by a bacteria. Most people get impetigo through skin-to-skin contact with someone who has it. It’s also possible to get it by using something infected with the bacteria.
Is treatment needed? Yes. To cure this infection, a child usually needs an antibiotic that you apply to your child’s skin, along with proper skin care.
Related AAD resource:
Keratosis pilaris
Contagious: No.
Is treatment necessary: No. This condition is completely harmless. Dermatologists offer treatment to teenagers and adults who dislike the way KP makes their skin look.
Related AAD resources:
Molluscum contagiosum

Contagious: Yes. Because this condition is contagious and tends to last for months, it’s important to take precautions to prevent your child from spreading the virus to you and others.
Is treatment necessary: Some children need treatment; others don’t. A board-certified dermatologist can tell you which is recommended for your child.
When a child has a healthy immune system, dermatologists often recommend letting the disease clear on its own. Clearing can take time. You may see new bumps for several months. As some bumps clear, new ones can appear. This cycle usually lasts about 6 to 18 months before the skin clears completely.
Related AAD resources:
Pityriasis rosea

Contagious: Pityriasis rosea is not thought to be contagious.
Is treatment needed? The rash will clear on its own, so it’s usually nothing to worry about. Still, it’s important to get diagnosed. It’s possible that the rash could be something other than pityriasis rosea.
Related AAD resource:
Scabies

Contagious: Yes.
Is treatment needed? Yes. The person diagnosed with scabies and everyone who has had close contact with that person need treatment. The medicine used to treat scabies is only available with a doctor’s prescription.
Related AAD resource
How to clear the bumps on your child’s skin
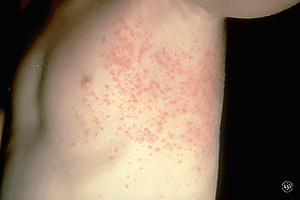
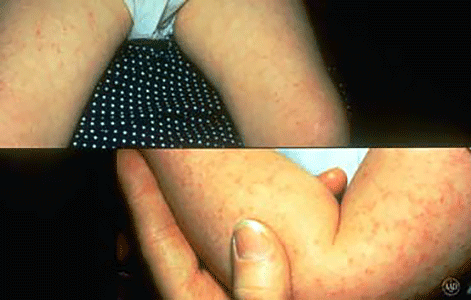
While some bumps will clear on their own, getting an accurate diagnosis is essential. It can be difficult to know what’s causing your child’s rash. Bumps on the skin can look alike. Could you tell the difference between long-lasting hives and atopic dermatitis? The pictures shown here look alike, don’t they?
It often takes years of in-depth medical training and experience to spot the differences. Your pediatrician or board-certified dermatologist can give you an accurate diagnosis. To become board certified, a dermatologist must know how to diagnosis and treat more than the 3,000 conditions that affect the skin.
Are all dermatologists board certified?
No. See what it takes to become board certified.

Images
2, 7, 10: Used with permission of DermNet New Zealand Image Library.
3,4: Getty Images
5: Image: J Am Acad Dermatol. 2013;69:736-41
References
Belazarian L, Lorenzo ME, et al. “Exanthematous viral diseases.” In: Wolff K, Goldsmith LA, et al. Fitzpatrick’s Dermatology in General Medicine (seventh edition). McGraw Hill Medical, New York, 2008: 1867-9.
Blauvelt A. “Pityriasis rosea.” In: Wolff K, Goldsmith LA, et al. Fitzpatrick’s Dermatology in General Medicine (seventh edition). McGraw Hill Medical, New York, 2008:362-6.
Gratten CEH, Black AK. “Urticaria and angioedema.” In: Bolognia JL, et al. Dermatology. (second edition). Mosby Elsevier, Spain, 2008: 261-75.
Habif TP, Campbell, JL, et al. “Impetigo.” In: Dermatology DDxDeck. Mosby Elsevier, China, 2006: Card#46.
McMichael A, Guzman Sanchez D, et al. “Folliculitis and the follicular occlusion tetrad.” In: Bolognia JL, et al. Dermatology. (second edition). Mosby Elsevier, Spain, 2008: 517-9.
Miller JI. “Diseases of the eccrine and apocrine sweat glands.” In: Bolognia JL, et al. Dermatology. (fourth edition). Elsevier, China, 2018:644.
Pigatto P, Martelli A, et al. “Contact dermatitis in children.” Ital J Pediatr. 2010 Jan 13;36:2.
Stone SP, Goldfarb JN, et al. “Scabies, other mites, and pediculosis.” In: Wolff K, Goldsmith LA, et al. Fitzpatrick’s Dermatology in General Medicine (seventh edition). McGraw Hill Medical, New York, 2008:2019-2032.
Tom W, Fallon Friedlander S. “Poxvirus infections.” In: Wolff K, Goldsmith LA, et al. Fitzpatrick’s Dermatology in General Medicine (seventh edition). McGraw Hill Medical, New York, 2008: 1911-13.
Zaenglein AL and Thiboutot DM. “Acne vulgaris.” In: Bolognia JL, et al. Dermatology. (second edition). Mosby Elsevier, Spain, 2008:500.